2017年九月 Aesthetic Plastic Surgery 論文
Capsular Contracture Rate After Breast Augmentation with Periareolar Versus Other Two (Inframammary and Transaxillary) Incisions: A Meta-Analysis
BACKGROUND:
Capsular contracture has been the most common complication of cosmetic breast augmentation. The effect of incision pattern on capsular contracture is still unclear. This meta-analysis demonstrates current evidence with regard to the comparison of capsular contracture rate between periareolar and other two (transaxillary and inframammary) incisions.
METHODS:
PubMed, EMBASE, and Cochrane databases were searched up to January 2017. The results of selected studies were meta-analyzed to obtain a pooled odds ratio of the effect of periareolar versus other two incision patterns (transaxillary or inframammary incision) of breast augmentation on capsular contracture rates. In addition, subgroup analyses were performed on periareolar versus transaxillary groups and periareolar versus inframammary groups with regard to capsular contracture rate.
RESULTS:
Seven comparative studies were selected and meta-analyzed. Five of the seven studies reported a higher rate of capsular contracture on patients with periareolar incisions. The results showed a significantly higher rate of capsular contracture with periareolar incisions compared with other two incisions (OR, 1.83; 95% CI, 1.06-3.15, p = 0.03). Subgroup results showed no significant difference of capsular contracture between periareolar incisions and transaxillary incisions (OR, 0.94; 95% CI, 0.52-1.64, p = 0.79) and showed a significantly higher rate of capsular contracture in periareolar incisions compared to inframammary incisions (OR, 1.91; 95% CI, 1.06-3.43, p = 0.03).
CONCLUSION:
The results of this meta-analysis demonstrate the contributing effects of periareolar breastaugmentation on the rate of capsular contracture. However, more studies with longer tracking periods and higher quality should be conducted to further verify this conclusion.
Capsular contracture has been the most common complication of cosmetic breast augmentation. The effect of incision pattern on capsular contracture is still unclear. This meta-analysis demonstrates current evidence with regard to the comparison of capsular contracture rate between periareolar and other two (transaxillary and inframammary) incisions.
METHODS:
PubMed, EMBASE, and Cochrane databases were searched up to January 2017. The results of selected studies were meta-analyzed to obtain a pooled odds ratio of the effect of periareolar versus other two incision patterns (transaxillary or inframammary incision) of breast augmentation on capsular contracture rates. In addition, subgroup analyses were performed on periareolar versus transaxillary groups and periareolar versus inframammary groups with regard to capsular contracture rate.
RESULTS:
Seven comparative studies were selected and meta-analyzed. Five of the seven studies reported a higher rate of capsular contracture on patients with periareolar incisions. The results showed a significantly higher rate of capsular contracture with periareolar incisions compared with other two incisions (OR, 1.83; 95% CI, 1.06-3.15, p = 0.03). Subgroup results showed no significant difference of capsular contracture between periareolar incisions and transaxillary incisions (OR, 0.94; 95% CI, 0.52-1.64, p = 0.79) and showed a significantly higher rate of capsular contracture in periareolar incisions compared to inframammary incisions (OR, 1.91; 95% CI, 1.06-3.43, p = 0.03).
CONCLUSION:
The results of this meta-analysis demonstrate the contributing effects of periareolar breastaugmentation on the rate of capsular contracture. However, more studies with longer tracking periods and higher quality should be conducted to further verify this conclusion.
中文簡譯導讀
此篇論文篇名為:Capsular Contracture Rate After Breast Augmentation with Periareolar Versus Other Two (Inframammary and Transaxillary) Incisions: A Meta-Analysis. 刊登在Aesthetic Plastic Surgery,主旨在討論不同切口(乳暈旁,腋下與胸下緣切口)在隆乳手術時的莢膜攣縮比例。是一篇大規模的統計 meta-analysis,統計了七個比較性的研究(comparative study),結果發現在這七個比較性研究中,有五個指出乳暈切口有較高的莢膜攣縮比例,整體而言,乳暈切口隆乳比其他切口隆乳(腋下與胸下緣)有較高的莢膜攣縮比例(Odds Ratio, 1.83, p=0.03)。而進一步的次分類分析則發現:
- 乳暈隆乳與腋下隆乳的莢膜攣縮比例無明顯差異 (Odds Ratio, 0.94, p=0.79)
- 乳暈隆乳比胸下緣隆乳有較高的莢膜攣縮比例 (Odds Ratio, 1.91, p=0.03)
吳至偉醫師經驗
隆乳術後的莢膜攣縮,讓許多醫師與女性朋友困擾,以目前的研究來說,以非乳暈的的切口,使用絨毛面果凍矽膠,將果凍矽膠放在胸大肌下,可以得到最低的莢膜攣縮比例,而這也是吳至偉醫師目前的隆乳常規使用方式。
隆乳關鍵14點

Willam Adams設計的隆乳關鍵14點,目的在減少隆乳時細菌感染與莢膜攣縮的機率〔見上圖的內文:Designed to minimize bacterial contamination and capsular contracture in breast augmentation procedure〕
而為了有效減少莢膜攣縮,世界知名的美國UT Southwestern乳房整形名醫William Adams M.D.在多年前發表論文強調隆乳手術中的關鍵14點,如果可全部做到即可有效的降低莢膜攣縮比例,這14點分別為
- 麻醉開始前給予靜脈注射預防性抗生素
- 避免乳暈旁切口
- 使用Nipple Shield〔註:指手術時以防水貼布將乳頭貼住,以減少乳頭分泌物造成之污染〕
- 仔細執行微創之手術剝離
- 避免切割進入乳腺組織
- 仔細執行止血
- 使用雙平面空間置放
- 剝離空間以優碘/抗生素之三合一製劑消毒
- 減少皮膚與義乳假體的接觸〔註:使用隆乳擠花袋Kellr Funnel〕
- 減少義乳假體曝露在外的時間
- 在植入義乳假體前更換乾淨的手套與器械
- 盡可能避免使用引流管〔註:引流管雖能引流血水,但也是潛在細菌從體外進入體內的路徑〕
- 傷口做多層次的縫合
- 將來有任何侵入性治療都需使用預防性抗生素〔例如:拔牙或蛀牙的處理〕
綜觀這14點,每一點對於預防莢膜攣縮都很重要,是吳醫師執行隆乳手術時一定會注意的關鍵且融入隆乳常規。其中第2點就強調避免使用乳暈切口,足見乳暈旁切口造成較高的莢膜攣縮是多數醫師的共識與經驗。

植入義乳假體時使用隆乳擠花袋〔Keller Funnel〕可減少皮膚與義乳假體的接觸
隆乳心得與趣談:「我是莢膜殺手?!」
這個月(2017-8)在門診諮詢幾位隆乳的女性朋友,意外發現我自己在她們心中有「莢膜殺手」稱號。談起莢膜,每個隆乳的女性與醫師大概都聞之色變,在吳醫師的行醫生涯中,也處理過大大小小各種程度不同的莢膜攣縮。是的,這個稱號吳醫師應該受之無饋,因為吳醫師總是很小心的進行無菌,精準,不流血的隆乳手術,加上選擇正確的矽膠、置放位置與切口,務求將莢膜攣縮的比例降到較低。下圖是2013年刊載於整形外科知名期刊PRS的論文,追蹤2560位隆乳者長達五年的結果,詳細比較了各種果凍矽膠置放方式與術後的狀況下,發生莢膜攣縮的比例。依統計結果,發生莢膜攣縮(包膜攣縮)主要的因素為「乳暈旁切口(Periareolar incision site),乳腺下置放(Subglanduar placement),光滑面矽膠(smooth surface),胸罩(surgical bra錯誤的壓迫),血腫(hematoma)等」。其中莢膜攣縮較低的是絨毛面果凍矽膠置放在胸大肌下(2-3%),較高的則是光滑面果凍矽膠置放在乳腺下(20%);而絨毛面置放在乳腺下與光滑面置放在胸大肌下,則有相近的莢膜攣縮比例(4-5%)。所以吳醫師在手術時,會盡量的採取非乳暈旁切口,將矽膠放在胸大肌下,做好止血,穿戴正確的術後胸罩,以達到較低的莢膜攣縮比例。
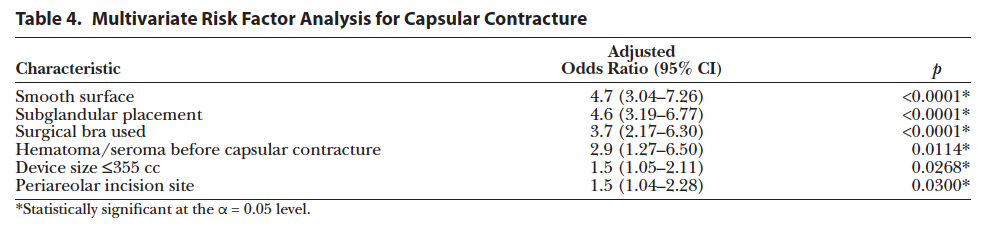
光滑面,乳腺下的置放為莢膜攣縮的風險因子中較高的兩項。
