義乳取出後如何完成隆乳重做(二次隆乳)? (Simultaneous Implant Removal with Fat Graft or Reimplantation)
有不少患者,因之前在其他地方接受義乳隆乳(果凍矽膠或鹽水袋),因觸感不好或莢膜攣縮而至吳醫師門診就診;這樣的狀況首先要評估莢膜攣縮的狀況,若是二度的莢膜攣縮,通常可以考慮不將義乳取出,直接以自體脂肪填補胸部較薄之處,讓胸部觸感更好一些,若是三度以上的莢膜攣縮,則通常有四種解決方式:
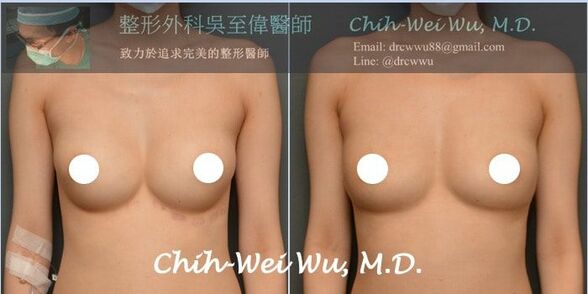
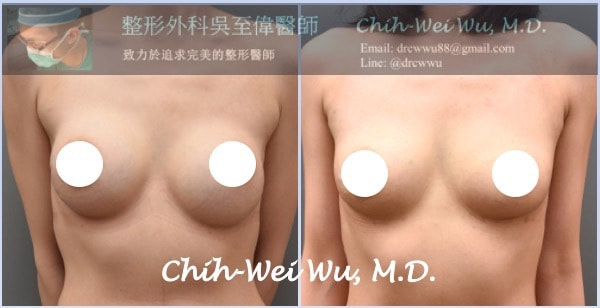
許多人因體質易排斥外來物,在經過多年的義乳產生問題後,希望能取出義乳,不再置入新的矽膠,這樣的考量則需接受第二種或第四種手術方式,但整體來說,我比較建議第二種方式(義乳取出,同時以自體脂肪完成重做)而不要單純取出不重建。可從腋下進行切口,以內視鏡剝離小空間,在移除果凍矽膠同時,保留莢膜組織並且不要破壞乳房的血液循環,以利自體脂肪隆乳的存活,在精密的手術技巧,搭配純化的脂肪與注射技術,經過一次的自體脂肪移植,多可以得到令人滿意的結果。此觀念於2009年克里醫師(Roger Khouri, M.D.)來台進行自體隆乳示範手術(Megavolume Fat Graft,吳至偉醫師當時為示範手術的Moderator)時即提出,在他的案例中,果凍矽膠取出後可同時移植400-500 c.c.的脂肪。下圖為二個義乳莢膜攣縮案例,經移除義乳後同時進行自體脂肪隆乳,術後六個月的結果*。
- 第一種隆乳重做(二次隆乳)方式:清除莢膜,義乳取出,同時改放置絨毛面果凍矽膠於肌肉雙平面下。
- 第二種隆乳重做(二次隆乳)方式:義乳取出後以自體脂肪隆乳的方式填補空間。
- 第三種隆乳重做(二次隆乳)方式:清除莢膜,義乳取出,同時以絨毛面果凍矽膠與自體脂肪移植完成複合式隆乳(hybrid breast augmentation)
- 第四種方式:義乳取出後不重建。
許多人因體質易排斥外來物,在經過多年的義乳產生問題後,希望能取出義乳,不再置入新的矽膠,這樣的考量則需接受第二種或第四種手術方式,但整體來說,我比較建議第二種方式(義乳取出,同時以自體脂肪完成重做)而不要單純取出不重建。可從腋下進行切口,以內視鏡剝離小空間,在移除果凍矽膠同時,保留莢膜組織並且不要破壞乳房的血液循環,以利自體脂肪隆乳的存活,在精密的手術技巧,搭配純化的脂肪與注射技術,經過一次的自體脂肪移植,多可以得到令人滿意的結果。此觀念於2009年克里醫師(Roger Khouri, M.D.)來台進行自體隆乳示範手術(Megavolume Fat Graft,吳至偉醫師當時為示範手術的Moderator)時即提出,在他的案例中,果凍矽膠取出後可同時移植400-500 c.c.的脂肪。下圖為二個義乳莢膜攣縮案例,經移除義乳後同時進行自體脂肪隆乳,術後六個月的結果*。
實際案例

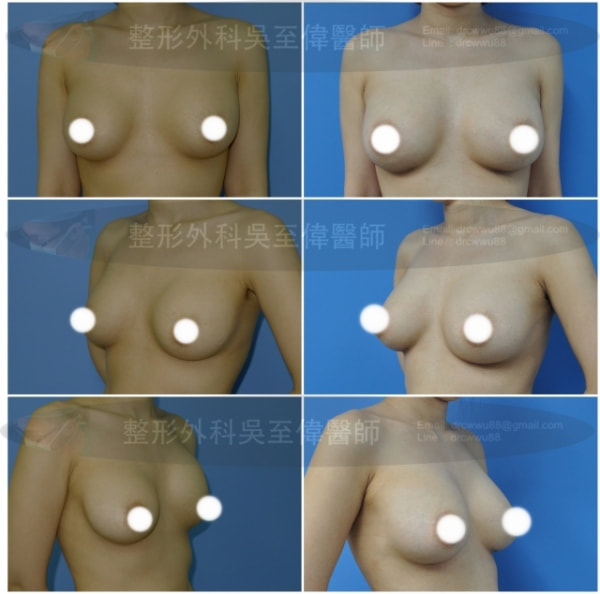
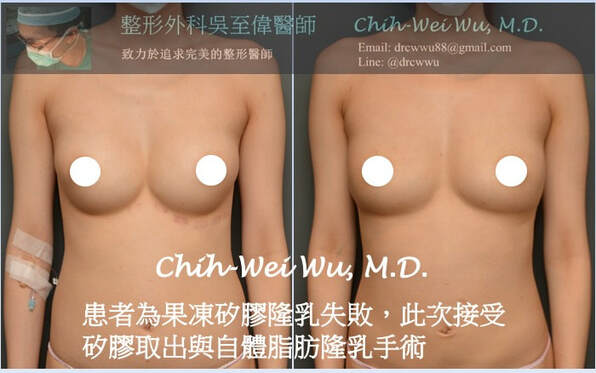
此患者為鹽水袋隆乳後多年破裂,此次接受經腋下義乳取出同時進行自體脂肪隆乳完成隆乳重做
此案例前次隆乳因空間過度往內側剝離而致明顯變形不好看,此次接受經腋下義乳取出同時進行自體脂肪隆乳完成隆乳重做。
此案例隆乳後多年因矽膠往下滑動而致明顯不對稱,此次接受經腋下義乳取出同時進行自體脂肪隆乳完成隆乳重做。
療程介紹
- 手術方式:矽膠或鹽水袋移除(經腋下/乳暈/或胸下緣皆可)+SAFELipo抽脂+自體脂肪移植隆乳。
- 適合者:假體隆乳後觸感不好,破裂或莢膜攣縮縮的果凍矽膠或鹽水袋。
- 麻醉方式:舒眠麻醉或全身麻醉手術。
- 手術時間:4小時。
- 術後照顧:可當天返家或住院一天。
- 恢復期:約一週
- 費用價格:請門診或來信諮詢
- 自體脂肪隆乳重做可能風險與後遺症:感染<1.1%,鈣化4.9%,脂肪壞死5.7%,腫塊1.1%,油泡等。
單純接受義乳取出時的建議
有些女性朋友在隆乳多年後,遇到莢膜攣縮、義乳移位、或長久不習慣外物在體內的困擾,想把義乳取出,吳醫師處理這類案例的經驗非常豐富,建議如下:
- 單純取出而不重做時,若原本胸部組織厚度夠,通常看不出凹陷,但假使原本胸部很平,則易因為凹陷而看出明顯變形。
- 單純義乳取出,不需清莢膜者:從原本隆乳切口進行即可;但若之前乳暈切口手術已達兩次(含)以上,則不建議再從乳暈切口。
- 需接受義乳取出加上同時清莢膜者:最好從乳下緣切口進行,一來避免手術時間過長,二來減少手術時的拉扯。若從乳暈進行莢膜攣縮清除手術,而不放置入新的果凍矽膠,術後造成乳頭凹陷的比例高達70%以上。
單純義乳取出案例

義乳取出前
|

義乳取出後
|
義乳取出後以果凍矽膠完成隆乳重做(二次隆乳)
部分女性朋友在義乳取出後選擇不再重做,或改以自體脂肪重做,但更多的人是選擇放入新的果凍矽膠,新一代的果凍矽膠自然度、觸感與安全性皆有大幅度的改善,可以考慮放入新一代的果凍矽膠完成隆乳重做。至於隆乳重做的費用,通常會較初次隆乳為高,但吳至偉醫師了解隆乳併發症的辛苦,對於果凍隆乳重做,除原本隆乳的費用外,僅酌收必要增加的麻醉與材料費用。
鹽水袋義乳位置過寬過高,手術方式為:果凍矽膠完成隆乳重做並將義乳集中與下調。

隆乳矽膠破裂與莢膜攣縮,手術方式為:莢膜清除手術+果凍矽膠完成隆乳重做。

果凍矽膠位置過低,手術方式為:果凍矽膠位置調整+胸下緣固定術。

此案例為義乳過度集中(symmastia,連通奶):左為術前,右為經空間調整縫合術後;連通奶的狀況特別容易發生在漏斗胸或胸骨凹陷的女性朋友,若有這種狀況,通常需將義乳取出,將內側空間做正確堅固的縫合,再將義乳置入,術後則需穿戴特製的胸衣至少兩個月。
最新論文:Aesthetic Surgery Journal 2015 Sep;35(7):819-29.
發表於Aesthetic Surgery Journal 2015年九月的論文,統計了80個在義乳取出時同時以自體脂肪隆乳完成隆乳重做,單側脂肪移植量為300至600毫升,所有的案例皆可一次完成,得到有效的隆乳重做;經過兩年的追蹤,產生油泡囊腫的比例為5.6%,感染的比例為1.25%,作者認為義乳取出時同時以自體脂肪隆乳完成隆乳重做是一項安全的手術。
Immediate Large-Volume Grafting of Autologous Fat to the Breast Following Implant Removal.
Abboud MH1, Dibo SA1.
BACKGROUND:
To optimize autologous breast augmentation, a simple and reproducible surgical approach that maximizes the volume of fat transferred to the breast while minimizing the number of sessions and the operating time is needed.
OBJECTIVES:
The authors describe a novel approach for large-volume fat grafting to the expanded skin and subcutaneous tissue of the breast immediately after explantation, exchanging the volume provided by the implants with transplanted fat in a single session.
METHODS:
Eighty patients (160 breasts) undergoing explantation and autologous fat transfer were evaluated in a prospective study. Fat was harvested with the lipomatic power-assisted liposuction machine (Lipomatic Eva SP, Euromi SA, Verviers, Belgium) and was injected with simultaneous vibration and tunnelization of the recipient site by means of the same machine with suction disabled. Changes in breast volume were measured in terms of bra cup size, and patients were monitored by mammography and ultrasonography. Patient satisfaction was assessed with a questionnaire administered 6 months postoperatively.
RESULTS:
Injected fat volumes ranged from 300 to 600 mL per breast. Operating times ranged from 45 to 90 minutes. For all patients, one injection session was sufficient to replace the volume of the previous implant. Patients were monitored for an average of 2 years, and complications included cyst formation in 9 of 160 breasts (5.6%) and infection in 2 breasts (1.25%).
CONCLUSIONS:Power-assisted transfer of autologous fat to the breast improves the ability of the recipient site to receive the graft and allows for explantation and fat transplantation in a single session. This approach is suitable for patients who desire a natural-appearing breast that is similar in volume to their previous implant.
To optimize autologous breast augmentation, a simple and reproducible surgical approach that maximizes the volume of fat transferred to the breast while minimizing the number of sessions and the operating time is needed.
OBJECTIVES:
The authors describe a novel approach for large-volume fat grafting to the expanded skin and subcutaneous tissue of the breast immediately after explantation, exchanging the volume provided by the implants with transplanted fat in a single session.
METHODS:
Eighty patients (160 breasts) undergoing explantation and autologous fat transfer were evaluated in a prospective study. Fat was harvested with the lipomatic power-assisted liposuction machine (Lipomatic Eva SP, Euromi SA, Verviers, Belgium) and was injected with simultaneous vibration and tunnelization of the recipient site by means of the same machine with suction disabled. Changes in breast volume were measured in terms of bra cup size, and patients were monitored by mammography and ultrasonography. Patient satisfaction was assessed with a questionnaire administered 6 months postoperatively.
RESULTS:
Injected fat volumes ranged from 300 to 600 mL per breast. Operating times ranged from 45 to 90 minutes. For all patients, one injection session was sufficient to replace the volume of the previous implant. Patients were monitored for an average of 2 years, and complications included cyst formation in 9 of 160 breasts (5.6%) and infection in 2 breasts (1.25%).
CONCLUSIONS:Power-assisted transfer of autologous fat to the breast improves the ability of the recipient site to receive the graft and allows for explantation and fat transplantation in a single session. This approach is suitable for patients who desire a natural-appearing breast that is similar in volume to their previous implant.
義乳取出同時進行脂肪移植完成隆乳重做主要研究
在2012年時,Boston 波士頓的乳房整形專家Daniel Del Vecchio發表在整形外科期刊PRS的論文即提到,將義乳取出時,可同時以自體脂肪完成重做。並可得到很好的結果。
"SIEF"--simultaneous implant exchange with fat: a new option in revision breast implant surgery.
Plast Reconstr Surg. 2012 Dec;130(6):1187-96. doi: 10.1097/PRS.0b013e31826d9c3c.
Del Vecchio DA1.
A technique of implant exchange is reported using recipient-site preexpansion followed by autologous fat transplantation to the breast in 12 consecutive patients with breast implants who desired implant removal. Recipient-site preexpansion, used 2 weeks before fat grafting, may have both practical and theoretical benefits in increasing the breast subcutaneous space and stimulating the recipient-site microcellular environment overlying the prosthetic implant, allowing the subcutaneous insertion of a sufficient core volume of donor graft at the time of prosthetic explantation. In the cases described, the postexplantation breast volume at 9 months to 1 year postoperatively by quantitative three-dimensional imaging was equal to or greater than the preexplantation composite volume of breast and implant. Preexpansion before implant exchange with fat affords a more abundant space, completely independent from the subglandular or submuscular planes. In this new space, the "third space" of the breast, it is possible to technically place graft into the breast subcutaneous tissue and alleviate breast asymmetry resulting from pocket distortions caused by capsular contracture or by implant pocket drift. Observing breast augmentation with implants and with fat grafting in the same patient affords a unique opportunity to analyze some of the key differences between the two techniques. Recipient-site preexpansion and simultaneous implant exchange with fat (SIEF) should be added to the list of applications where fat grafting to the breasts may have early clinical utility and portends the use of fat used in conjunction with breast implants to achieve better patient outcomes.
Del Vecchio DA1.
A technique of implant exchange is reported using recipient-site preexpansion followed by autologous fat transplantation to the breast in 12 consecutive patients with breast implants who desired implant removal. Recipient-site preexpansion, used 2 weeks before fat grafting, may have both practical and theoretical benefits in increasing the breast subcutaneous space and stimulating the recipient-site microcellular environment overlying the prosthetic implant, allowing the subcutaneous insertion of a sufficient core volume of donor graft at the time of prosthetic explantation. In the cases described, the postexplantation breast volume at 9 months to 1 year postoperatively by quantitative three-dimensional imaging was equal to or greater than the preexplantation composite volume of breast and implant. Preexpansion before implant exchange with fat affords a more abundant space, completely independent from the subglandular or submuscular planes. In this new space, the "third space" of the breast, it is possible to technically place graft into the breast subcutaneous tissue and alleviate breast asymmetry resulting from pocket distortions caused by capsular contracture or by implant pocket drift. Observing breast augmentation with implants and with fat grafting in the same patient affords a unique opportunity to analyze some of the key differences between the two techniques. Recipient-site preexpansion and simultaneous implant exchange with fat (SIEF) should be added to the list of applications where fat grafting to the breasts may have early clinical utility and portends the use of fat used in conjunction with breast implants to achieve better patient outcomes.
延伸閱讀
門診時間
*吳醫師致力於提供完善的整形資訊,但網站資訊無法做為診斷、醫療之依據,網站案例亦為個別案例,實際效果因人而異,任何手術與醫療行為均有其潛在風險,於進行任何治療之前,應與專業醫師諮詢與溝通,再選擇適合自己的治療!
